
Overview
Long relegated to the rear-view mirror of drug trends, psilocybin-containing mushrooms, also known as “magic mushrooms,” have made a strong comeback in the last 5 years. Psilocybin and psilocybin mushrooms were placed on Schedule 1 under the Controlled Substances Act of 1970, de facto defining them as having a high potential for abuse and no accepted medical use. As it turns out, neither of these descriptions is true.
The major varieties of Psilocybe cubensis are hallucinogenic mushrooms of moderate potency, naturally occurring in tropical and subtropical areas throughout the world and easily cultivated from spores nearly everywhere.
Importantly, psychedelic mushrooms are no longer the sole purview of naturalists seeking enlightenment, connoisseurs of recreational hallucinogens, or the weekend I’ll-try-anything-once club. Psilocybin mushrooms are on the radar screen of drug companies as an FDA-designated “breakthrough treatment” for depression and in preliminary clinical trials for smoking cessation and other addictive behaviors. They can also be found in psychiatrist offices for psychedelic-assisted therapy, in therapy centers and psychedelic retreats/spas staffed by certified lay hallucinogen facilitators, in unregulated web stores and neighborhood head shops, and via health food stores and the internet as supplements for anyone seeking more calmness and clarity in their lives.
Clinical research into the application of psilocybin in medicine is expanding rapidly. The downside is that results are exaggerated and embellished into miracle-drug status by word-of-mouth and social media testimonials. If you haven’t yet encountered anyone using psilocybin mushrooms, you will soon.
Pharmacology of Psilocybin
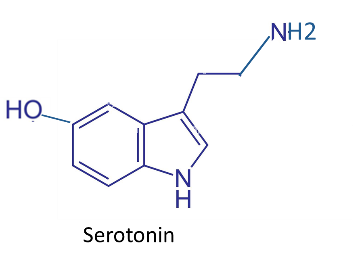
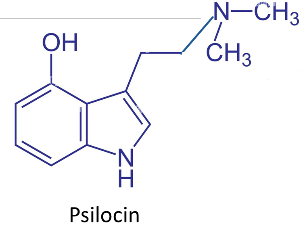
The active principle in the psilocybin mushroom is the chemical psilocybin, which undergoes a very rapid “first pass” metabolism after ingestion to its active form, psilocin.
Psilocin is chemically related to serotonin and can activate all of the various serotonin receptors.
Since psilocin is lipophilic, it readily passes the blood-brain barrier, where activation specifically of 5HT-2A receptors is responsible for the hallucinogenic effects. Nausea and vomiting are common adverse effects because serotonin is richly represented in the GI tract. Cross-talk among neurotransmitters results in minor activation of the sympathetic nervous system, giving elevated heart rate and blood pressure, tremor, and sometimes other dyskinesias.
Onset of effect is 30-45 minutes, peak at about 2 hours, and duration about 4 to 7 hours. Psilocin itself is subsequently metabolized with an average half-life of about 2-3 hours.
Psilocybin can be synthetically prepared, but most users ingest intact mushrooms, usually dried to preserve them. Dried mushrooms contain somewhere between 0.5 and 2% psilocybin, with 1% content being the default assumption. Therefore, 1 gram of dried mushroom delivers approximately 10 mg of psilocybin, the low end of psychedelic dosing. Dose is variously expressed as total mg amount or mg/kg of psilocybin or as grams of dried mushroom.
Dose-Related Effects and Psilocybin Microdosing
What the person experiences psychically is related to how much mushroom they ingest. The classic hallucinogenic experience is induced by 10 mg of psilocybin, and it ramps up as the dose increases to 30-40 mg. The usual range is 25-40 mg of psilocybin (approximately 0.3-0.4 mg/kg) delivered in 2.5-4 grams of dried mushroom. As a psychedelic, it is said to be more strongly visual than LSD, with enhanced color and geometric patterns like a traditional Indian blanket. It is also more emotionally intense, with feelings ranging from euphoria, overwhelming joy, gratitude, and harmony to dysphoria and focus on the GI upset, to fear and paranoia, possibly resulting in self-harm behaviors. Perceptual alterations increase with the dose, ranging from subtle, such as time distortion, to profound, such as dissolution of self and mystical union with the universe.
Measurable physical effects during intoxication include nausea and vomiting, tachycardia, elevated blood pressure, and sometimes mydriasis.
Sub-threshold dosing, also known as microdosing, is purported to enhance focus, memory, mood, and immune defense without noticeable perceptual changes. Microdosing is regular ingestion several times a week of a very low dose of psilocybin that does not cause noticeable effects, e.g., 0.1 to 0.3 grams of mushroom (1-3 mg psilocybin). It is an increasingly popular nootropic supplement. There are anecdotal reports of enhanced well-being, creativity, and cognitive function, but the only attempt at a double-blind assessment indicated that the placebo effect was responsible for perceived benefits.
Unusual Therapeutic Mechanism in Psychiatry
Psilocybin has an unusual hypothetical mechanism for its effectiveness as an antidepressant or as an adjunctive tool in the treatment of alcohol or nicotine use disorders. This is not a daily dose of a pharmacologically active drug that alters neurotransmission. It is one or two doses of a mild-altering drug that are preceded by, accompanied by, and followed up with directed counseling.
The current theory involves a particular neural network in the brain that helps shape and control the individual’s sense of self and their relationship to the various aspects of their past, present, imaginary, and future life as more or less a cohesive internal narrative. Psilocybin and other psychedelics can temporarily disrupt this “Default Mode Network” and de-synchronize the connections that normally co-activate. This enhances the network’s plasticity, making it possible to reorganize in a different and more adaptive way. With “before, during, and after” professional guidance to take advantage of this openness to new perspectives about the self, the patient can make lasting changes in thoughts, emotions, and behaviors. This is psilocybin’s utility in the treatment of depression and at least partial success in smoking cessation and alcohol sobriety. To date, the clinical findings are not strong for other addictive behaviors.
This proposed mechanism also sheds light on the “bad trip” reactions that people can experience when they initially use psilocybin mushrooms recreationally or use them without adequate psychological preparation. Psychoactive co-ingestants may also be involved in an adverse experience, as well as improper dosing or contaminated drugs. The hallucinations and perceptual disturbances involving the dissolution of self can be frightening and produce anxiety or panic that may bring them to the Emergency Department. These adverse effects are much less common during assisted therapy.
Available Sources and Surprise Appearances
Psilocybin is typically ingested by eating dried or possibly fresh mushrooms. Where do these come from, since the ‘shrooms are currently illegal except in 2 western states? Because selling Psilocybe cubensis spores is legal, complete grow kits from many suppliers are available on trusted, giant web merchant sites. They describe themselves obliquely, for example, “The Micro Magical 3 lb All-in-One Mushroom Grow Bag | Harvest Your Own Happiness | Discover The Magic of Growing Mushrooms.”
A tea may be brewed, or it may be eaten with food to help mask the bitter taste. In placebo-controlled clinical trials, the psilocybin and placebo are packed into gelatin capsules.
Recently, “mushrooms” as a general class have emerged in “edibles” such as chocolate bars and gummy candies, many ostensibly to facilitate microdosing or to produce a “legal psychedelic high.” However, these products are usually labeled as an extract of other mushroom species, which also have some reputation for nootropic or mind-altering properties, such as Lions Mane, Turkey Tail, or Amanita muscaria.
Not surprisingly, chemical analysis of some of these products tells a different story. Those specifically claimed to contain Amanita muscaria had neither muscimol nor ibotenic acid in them. Agents detected included illegal psilocybin itself, other psilocin prodrugs, a variety of active serotonergic tryptamines related to psilocybin, mitragynine (Kava, sedative and anxiolytic), ephedrine and phenethylamine (sympathomimetics), and designer drugs related to MDMA (hallucinogenic amphetamines). The only thing certain about these nootropic mushroom products is their uncertainty and high risk of inaccurate and misleading labeling.
Psilocybin Tolerance, Dependence, and Safety
Contrary to its Schedule 1 status, psilocybin is not a drug that has a high potential for abuse, but it can be misused. Tolerance to psilocybin may occur in users partaking more than once a week, who experience diminishing effects and need to increase the dose. Tolerance quickly wanes with abstinence. Physical dependence and withdrawal, on the other hand, have not been reported. There have been no drug-related fatalities when psilocybin was ingested as the sole ingestant. However, injury and death have been reported from panicked behavioral responses to the experience, such as jumping out of a window. When compared to other drugs of abuse, psilocybin mushrooms show the lowest level of harm.
Psilocybin should not be used in women who are pregnant or breastfeeding because there is insufficient research in this population to assess safety. There are relative contraindications for those who take atypical antipsychotics and certain antidepressants that may block the desired hallucinogenic effects. This is because people taking these medicines or having these conditions are specifically excluded from clinical trials, again offering insufficient safety information in these populations. MAO inhibitors prevent one of the major enzyme reactions that inactivate psilocin, thereby boosting its blood level, prolonging its half-life, and may increase its risk.
Treatment of Adverse Reactions
The majority of psilocybin users who present to the Emergency Department have intense anxiety or panic and tachycardia. Only a few cases of serious illness have been reported, and most are suspected to be multiple-agent ingestions. Serious features have included hallucinations, seizures, coma, hyperthermia, and Acute Kidney Injury. Treatment for psilocybin intoxication is symptomatic and supportive; there is no specific antidote. Benzodiazepines are generally used for patients presenting with agitation, hallucinations, seizures, tremor, or dyskinesia, and escalation of care follows usually accepted treatment paths.
Call to Action
For patient-specific guidance, please contact the Missouri Poison Center’s dedicated line for healthcare professionals at 1-888-268-4195. Our specially trained nurses, pharmacists, and toxicologist can offer information on psilocybin mushroom ingestion and provide the most up-to-date information regarding exposure and treatment.
You can check out our article on magic mushrooms for the general public.